Case studies
Social Movement Action Framework
Promoting healthy public policy through mobilized collective actions
Queen’s Park on the Road and Queen’s Park Day are two events in which RNAO members meet with members of provincial parliament (MPPs) from all of the political parties to promote healthy public policy and nursing services. through individual and collective actions. Learn more in this case study.
Through two annual initiatives – Queen’s Park on the Road and Queen’s Park Day – RNAO members meet with members of provincial parliament (MPPs) from all of the political parties to promote healthy public policy and nursing services. Through direct engagement and advocacy with MPPs, RNAO has mobilized collective action for policy initiatives addressing areas such as poverty reduction, the use of pesticides for cosmetic use, promoting refugee health and protecting the safety and security of residents in long-term care (Grinspun et al., 2018a).

Mobilizing community engagement to sustain a childhood obesity prevention initiative
Multiple communities mobilized to sustain a childhood obesity prevention program through targeted individual and collective action. Read more in this case study.
A community initiative called Sustainable Childhood Obesity Prevention through Community Engagement (SCOPE) provides an example of collective action in the context of public health.
In the SCOPE public health initiative, the community formed a coalition with local partners such as libraries and primary care offices to take collective action for the prevention of childhood obesity. Together, they participated in a range of collective action activities, including: presentations and events promoting healthy eating choices, stakeholder engagement, resource development and policy and practice change (Kennedy et al., 2019a).

Building a global collective identity to advance knowledge uptake and sustainability - the RNAO Best Practice Spotlight Organization (BPSO) Program
RNAO's Best Practice Spotlight Organization (BPSO) program has integrated a collective identity of knowledge champions to advance evidence uptake and sustainability.
|
The Best Practice Spotlight Organization® (BPSO®) Program (https://rnao.ca/bpg/bpso) has global reach and impact that is sustained by many factors, including the development of collective identity that promotes an evidence-based culture. The BPSO logo, as a tangible representation of a collective identity, is displayed in individual sites to indicate they are BPSO units. This visibility motivates and inspires nurses and other staff to use best practice guidelines (BPG) to support the health and well-being of staff, patients/persons and their families. Participation and membership in the international BPSO network further the ties and pride of BPSO and builds the collective identity (Grinspun & Bajnok, 2018).
Within organizations, individual BPSOs nurture Best Practice (BP) Champions (https://rnao.ca/bpg/get-involved/champions) who take on leadership roles to support the planning, implementation, evaluation and sustainability of BPGs. Nurses and other staff members develop a collective identity based on a culture of integrating evidence-based practice to achieve excellence in care. The visibility of BP Champions is seen when staff where BPSO-branded clothing items, and pins that are awarded at the completion of the Best Practice Champions’ training workshop (see the examples below of social media posts of BPSO-branded t-shirts and a pinning ceremony of new champions by RNAO CEO, Dr. Doris Grinspun) (Grinspun & Bajnok, 2018). |

Knowledge-to-Action Framework
Overcoming barriers to evidence-based practice – Lessons learned from DongZhiMen Hospital and Beijing University of Chinese Medicine (BUCM) School of Nursing
DongZhiMen Hospital and Beijing University of Chinese Medicine (BUCM) School of Nursing are international BPSOs in Beijing, China. Staff at the sites identified barriers to the use of evidence in practice including heavy workloads, cultural differences and reluctant attitudes about using evidence to inform practice.
DongZhiMen Hospital and Beijing University of Chinese Medicine (BUCM) School of Nursing are international BPSOs in Beijing, China. They identified barriers to the use of evidence in practice including heavy workloads, cultural differences and reluctant attitudes about using evidence to inform practice. The assessment and identification of barriers allowed change teams to develop effective strategies for implementation with the input of stakeholders.
For example, for the implementation of the RNAO best practice guideline Assessment and management of foot ulcers for people with diabetes, barriers included
- nursing shortages across China,
- a lack of training to support the development of knowledge and skills in evidence-based nursing practice,
- the costs of guideline implementation. and
- practice recommendations that exceeded local nursing scope.
SOURCE: Transforming Nursing Through Knowledge, 2018.

Evaluating the impact of implementing the Person- and Family-Centred Care Best Practice Guideline at Spectrum Health Care
Spectrum Health Care, a Best Practice Spotlight Organization® (BPSO®) and home health organization, evaluated care outcomes after implementing the Person- and Family-Centred best practice guideline (BPG).
Spectrum Health Care (Spectrum), an RNAO Best Practice Spotlight Organization® (BPSO®), is a home health organization with more than 200 nursing staff across three locations in the province of Ontario, Canada.
Spectrum chose to implement the 2015 Person- and Family-Centred Care (PFCC) Best Practice Guideline (BPG) to enhance person- and family-centred care and to reduce complaints regarding care. Members of the senior leadership team at Spectrum Health Care led implementation together with Spectrum’s Patient and Family Advisory Council.
To support the practice change, Spectrum used the following implementation interventions:
- Conducting a gap analysis to determine the knowledge/practice gap;
- Holding education sessions for staff on person- and family-centred care best practices;
- Revising their care processes to include review of care plans with the person and/or members of their family
- Surveying staff members on their attitudes about person- and family-centred care via surveys
- Developing staff education on communication strategies to support the assessment of a person’s care needs and care plans.

After implementing these interventions, Spectrum assessed the number of complaints received from persons receiving care per 1,000 care visits and compared that to their baseline.
They found a decrease of 42 per cent of complaints from persons received over an 18-month time period at one of the sites that was implementing the PFCC BPG at Spectrum Health Care.
At another site, an 80 per cent reduction in complaints was found following the staff education intervention.
Data analyses overall indicated that the implementation of the PFCC BPG was highly successful in reducing persons' complaints regarding care.
Read more about Spectrum Health care’s results of implementing the PFCC BPG here: Slide 2 (rnao.ca)

Sustaining the Assessment and Management of Pain Best Practice Guideline across a multi-site long-term care home
The Region of Peel, a Best Practice Spotlight Organization® (BPSO®), has sustained the implementation of the Assessment and Management of Pain best practice guideline (BPG) for almost a decade.
The Region of Peel, an RNAO Best Practice Spotlight Organization® (BPSO®) started implementing the RNAO Assessment and Management of Pain best practice guideline (BPG) in 2014 and has sustained its use since then. For example, in their 2019 BPSO annual report, they cited a continuous downward trend in the number of clients who reported a worsening of their pain. Pain experienced by the residents was better controlled, and the staff was found to assess, identify, and manage pain better by using the BPG.
Their keys to success include:
- building on what works (for example, existing practices and policies)
- empowering champions and growing their champion network
- involving residents and families
- gaining support from leaders and partners including RNAO, Peel of Region Leadership, Health Quality Ontario).
- collaborating with an interdisciplinary team
- conducting a formal sustainability evaluation
To learn more about The Region of Peel’s journey in sustaining the use of the Assessing and Managing Pain BPG, along with other BPGs, check out this webinar.

Engaging Persons with Lived Experiences
Holland Bloorview Kids Rehabilitation Hospital: Co-designing change through the active engagement of persons with lived experience
A case study from Holland Bloorview Kids Rehabilitation Hospital focused on engaging persons with lived experience in a change process.
Holland Bloorview Kids Rehabilitation Hospital (hereafter referred to as Holland Bloorview) is a designated Best Practice Spotlight Organization® (BPSO®) in Toronto, Ontario, Canada. Holland Bloorview has an award-winning Family Leadership Program (FLP), through which family leaders partner with the organization and the Bloorview Research Institute to co-design, shape, and improve services, programs, and policies. Family leaders are families and caregivers who have received services at Holland Bloorview, and have lived experiences of paediatric disability. Family leaders’ roles include being a mentor to other families, an advisor to committees and working groups, and faculty who co-teach workshops to students and other families.
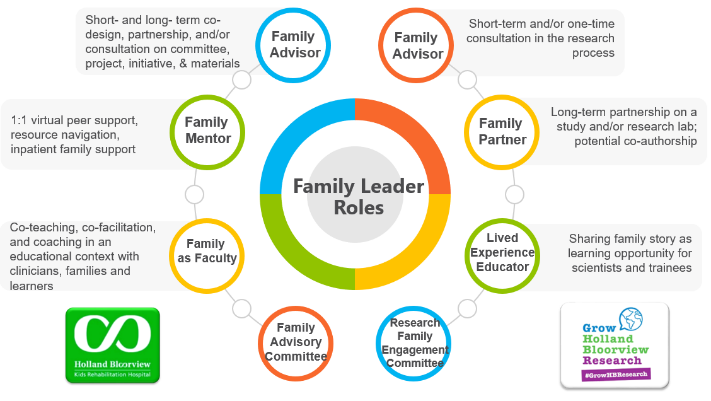
Family Leader Roles at Holland Bloorview. Photo provided with permission by Holland Bloorview Kids Rehabilitation Hospital.
The ENFit™ Working Group is an example of a successful implementation co-design process within Holland Bloorview. The ENFit™ Working Group is an interprofessional team working on the adoption of a new type of connection on products used for enteral feeding [feeding directly through the stomach or intestine via a tube]. By introducing the ENFit™ system, a best practice safety standard, the working group plans to reduce the risk of disconnecting the feeding tube from other medical tubes, and thus decrease harm to children and youth who require enteral feeding.

Family Partnering with the EnFit Working Group. Photo provided with permission by Holland Bloorview Kids Rehabilitation Hospital.
The working group invited a family member and leader whose son had received services at Holland Bloorview. This family member had significant lived experience with enteral feeding management, enteral medication administration, and other complexities associated with enteral products. During the meetings, great attention was given to the potential impacts on persons and families. The group engaged the family member by:
- co-creating the implementation plan
- involving them in a failure mode affects analysis, which highlighted the impact of the feeding tube supplies on transitions to home, school, and other care settings
- working with the family member to advocate for safe transitions within the provincial pediatric system, which led to the development of the Ontario Pediatric ENFit™ Group
To learn more about Holland Bloorview’s experience in partnering with families in a co-design process, watch their 38-minute webinar: The Power of Family Partnerships.

Engaging Patient Family Advisors to advance guideline implementation at Scarborough Health Network
A case study about the integration of patient family advisors at Scarborough Health Network to enhance community engagement and health equity.
Scarborough Health Network (SHN) (Home - Scarborough Health Network (shn.ca) is an organization pursuing Best Practice Spotlight Organization® (BPSO®) designation in Scarborough, Ontario, Canada. Patient Family Advisors (PFAs) are a vital part of SHN’s philosophy of care, representing the diverse community SHN serves. A key element of the PFA role is sharing lived experiences with SHN staff and the Scarborough community.
SHN has demonstrated commitment to the role of PFAs within their organization by creating a new department for health equity, patient and community engagement (HEPCE). This department focuses on:
- recruiting, onboarding, managing, recognizing and retaining PFAs
- educating staff on best practices related to engaging with PFAs
During recruitment and onboarding, the HEPCE and current PFAs educate potential PFAs about the role’s scope and expectations. All PFAs are also provided with information on how to share their patient or caregiver story with their audience.
PFAs have played an important role in SHN’s BPSO committee. Indeed, one PFA has been integral to the process of recruiting and engaging champions at SHN throughout the COVID-19 pandemic’s health human resources (HHR) crisis. Their role has included participating in champions’ virtual drop-in sessions (2020-2021) and in-person roadshows (2022).
Champion roadshows are events during, which SHN practice leaders and PFAs promote the BPSO program, share best practice guidelines and recruit champions around the organization, without asking busy staff members to leave their units.
The PFA also supported the recruitment and engagement of champions by:
- collaborating with other champions and working group members to plan champions’ drop-in sessions and roadshows
- working alongside the team to plan safe spaces for staff and PFAs to share their stories
- sharing stories of positive experiences with staff members in relation to the impact of best practices (for example, RNAO’s Person and Family Centred-Care best practice guideline) on their experience
Staff members have reported being motivated to become best practice champions after attending a champion’s roadshow. SHN has also consistently gained champions during the HHR crisis and maintains at least 15 per cent of nursing staff as best practice champions.
The PFA’s role was vital to demonstrating the lasting impact of best practices. They have expressed feeling empowered by their role in BPSO work, expressing that the work helped them find their voice and become part of the movement to promote and implement best practices.
Overall, PFAs play an essential – and dual – role in supporting the implementation of best practices at SHN. In line with person- and family-centred care, PFAs assume an outward-facing role in shaping the implementation of best practices and SHN’s values. In addition, they also act in an inward-facing role to support the bolstering of champions.
To learn more about the PFA role at SHN, please visit the following link: Patient Family Advisors.
Shared with permission by Scarborough Health Network

Co-designing change through the active engagement of persons with lived experience - Holland Bloorview Kids Rehabilitation Hospital
Case study - Holland Bloorview
Holland Bloorview Kids Rehabilitation Hospital (Holland Bloorview) is a designated Best Practice Spotlight Organization® (BPSO®) in Toronto, Canada. Holland Bloorview has an award-winning Family Leadership Program (FLP), through which family leaders partner with the organization and the Bloorview Research Institute to co-design, shape and improve services, programs and policies.
These family leaders are families and caregivers who have received services at Holland Bloorview and have lived experiences of paediatric disability. Their roles include mentoring other families, acting as advisors to committees and working groups, and co-teaching workshops to students and other families.
One example of a successful implementation co-design within Holland Broadview is the ENFit™ Working Group. This interprofessional team works on the adoption of a new type of connection on products used for enteral feeding – or feeding directly through the stomach or intestine via a tube. By introducing the ENFit™ system, a best practice safety standard, the working group plans to reduce the risk of disconnecting the feeding tube from other medical tubes. This in turn decreases harm to children and youth who require enteral feeding.
The working group invited a family member and leader whose son had received services at Holland Bloorview. This family member had significant lived experience with enteral feeding management, enteral medication administration, and other complexities associated with enteral products. During the meetings, the potential impacts on persons and families were emphasized. The working group engaged the family member by:
- co-creating the implementation plan
- involving them in a failure mode and effects analysis highlighting the impact of the feeding tube supplies on transitions to home, school and other care settings
- working with the family member to advocate for safe transitions within the provincial pediatric system, which led to the development of the Ontario Pediatric ENFit™ Group
To learn more about Holland Bloorview’s experience in partnering with families in a co-design process, watch their 38-minute webinar: The Power of Family Partnerships
Shared with permission from Holland Bloorview
