Case studies
Social Movement Action Framework
Building a global collective identity to advance knowledge uptake and sustainability - the RNAO Best Practice Spotlight Organization (BPSO) Program
RNAO's Best Practice Spotlight Organization (BPSO) program has integrated a collective identity of knowledge champions to advance evidence uptake and sustainability.
|
The Best Practice Spotlight Organization® (BPSO®) Program (https://rnao.ca/bpg/bpso) has global reach and impact that is sustained by many factors, including the development of collective identity that promotes an evidence-based culture. The BPSO logo, as a tangible representation of a collective identity, is displayed in individual sites to indicate they are BPSO units. This visibility motivates and inspires nurses and other staff to use best practice guidelines (BPG) to support the health and well-being of staff, patients/persons and their families. Participation and membership in the international BPSO network further the ties and pride of BPSO and builds the collective identity (Grinspun & Bajnok, 2018).
Within organizations, individual BPSOs nurture Best Practice (BP) Champions (https://rnao.ca/bpg/get-involved/champions) who take on leadership roles to support the planning, implementation, evaluation and sustainability of BPGs. Nurses and other staff members develop a collective identity based on a culture of integrating evidence-based practice to achieve excellence in care. The visibility of BP Champions is seen when staff where BPSO-branded clothing items, and pins that are awarded at the completion of the Best Practice Champions’ training workshop (see the examples below of social media posts of BPSO-branded t-shirts and a pinning ceremony of new champions by RNAO CEO, Dr. Doris Grinspun) (Grinspun & Bajnok, 2018). |

Building a collective identity to foster an anti-bullying culture
As part of a school anti-bullying campaign for children of military families in the United States, social movement participants used collective identity to promote anti-bullying messages. Read more in this case study.
As part of a grassroots anti-bullying campaign for children of military families in schools in the United States, social movement participants used collective identity to promote anti-bullying messages. Collective identity activities taken by school staff, parents and community members to promote the message "Because Nice Matters" included:
- designing and using posters, artwork and t-shirts to publicize their communication messages
- selecting and using the colours black and purple to unify their campaign
- engaging staff and students in the initiative
- having local businesses wear t-shirts with anti-bullying messaging as a sign of community support (de Pedro et al., 2017).

Guiding best practice guidelines (BPG) implementation with BPSO implementation teams
To support the effective implementation of BPGs, Best Practice Spotlight Organizations® (BPSOs®) create change teams that operate as core leadership structures to support evidence uptake and sustainability. Learn more in this case study.
To support the effective implementation of BPGs, Best Practice Spotlight Organizations® (BPSOs®) create change teams that operate as core leadership structures to support evidence uptake and sustainability. Their roles in the core leadership structure can include:
- selecting recommendations
- developing an action plan
- mobilizing implementation strategies
- supporting adherence to a practice change
- engaging in monitoring and evaluation activities
- taking active steps to support sustainability
As champions, one role of BPSOs is to compare their current practice to the guideline recommendations to see how the current practice can be maintained, strengthened or changed. Taking a “can do” attitude, they actively collaborate with their peers throughout the change process, and value and welcome their input and ideas. They take on leadership roles to support evidence-based practice change in collaboration with nurses, other staff and others (Bajnok et al., 2018a).

Knowledge-to-Action Framework
Sustaining the Assessment and Management of Pain Best Practice Guideline across a multi-site long-term care home
The Region of Peel, a Best Practice Spotlight Organization® (BPSO®), has sustained the implementation of the Assessment and Management of Pain best practice guideline (BPG) for almost a decade.
The Region of Peel, an RNAO Best Practice Spotlight Organization® (BPSO®) started implementing the RNAO Assessment and Management of Pain best practice guideline (BPG) in 2014 and has sustained its use since then. For example, in their 2019 BPSO annual report, they cited a continuous downward trend in the number of clients who reported a worsening of their pain. Pain experienced by the residents was better controlled, and the staff was found to assess, identify, and manage pain better by using the BPG.
Their keys to success include:
- building on what works (for example, existing practices and policies)
- empowering champions and growing their champion network
- involving residents and families
- gaining support from leaders and partners including RNAO, Peel of Region Leadership, Health Quality Ontario).
- collaborating with an interdisciplinary team
- conducting a formal sustainability evaluation
To learn more about The Region of Peel’s journey in sustaining the use of the Assessing and Managing Pain BPG, along with other BPGs, check out this webinar.

Engaging Persons with Lived Experiences
Holland Bloorview Kids Rehabilitation Hospital: Co-designing change through the active engagement of persons with lived experience
A case study from Holland Bloorview Kids Rehabilitation Hospital focused on engaging persons with lived experience in a change process.
Holland Bloorview Kids Rehabilitation Hospital (hereafter referred to as Holland Bloorview) is a designated Best Practice Spotlight Organization® (BPSO®) in Toronto, Ontario, Canada. Holland Bloorview has an award-winning Family Leadership Program (FLP), through which family leaders partner with the organization and the Bloorview Research Institute to co-design, shape, and improve services, programs, and policies. Family leaders are families and caregivers who have received services at Holland Bloorview, and have lived experiences of paediatric disability. Family leaders’ roles include being a mentor to other families, an advisor to committees and working groups, and faculty who co-teach workshops to students and other families.
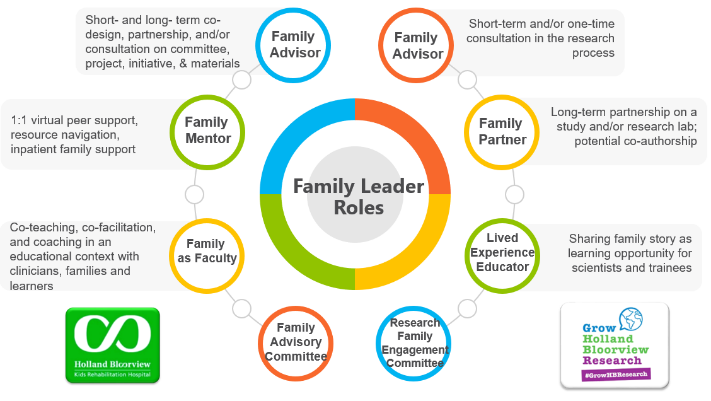
Family Leader Roles at Holland Bloorview. Photo provided with permission by Holland Bloorview Kids Rehabilitation Hospital.
The ENFit™ Working Group is an example of a successful implementation co-design process within Holland Bloorview. The ENFit™ Working Group is an interprofessional team working on the adoption of a new type of connection on products used for enteral feeding [feeding directly through the stomach or intestine via a tube]. By introducing the ENFit™ system, a best practice safety standard, the working group plans to reduce the risk of disconnecting the feeding tube from other medical tubes, and thus decrease harm to children and youth who require enteral feeding.

Family Partnering with the EnFit Working Group. Photo provided with permission by Holland Bloorview Kids Rehabilitation Hospital.
The working group invited a family member and leader whose son had received services at Holland Bloorview. This family member had significant lived experience with enteral feeding management, enteral medication administration, and other complexities associated with enteral products. During the meetings, great attention was given to the potential impacts on persons and families. The group engaged the family member by:
- co-creating the implementation plan
- involving them in a failure mode affects analysis, which highlighted the impact of the feeding tube supplies on transitions to home, school, and other care settings
- working with the family member to advocate for safe transitions within the provincial pediatric system, which led to the development of the Ontario Pediatric ENFit™ Group
To learn more about Holland Bloorview’s experience in partnering with families in a co-design process, watch their 38-minute webinar: The Power of Family Partnerships.
