Applying the Knowledge-to-Action Framework to reduce wound infections at Perley Health

Perley Health is a designate Long-Term Care Best Practice Spotlight Organization® (BPSO®) which demonstrates a strong commitment to providing evidence-based care. During the pandemic, the team identified skin and wound infection as a clinical concern among their residents. Consistent with the literature, residents at Perley Health experiencing comorbid medical conditions such as frailty, diabetes, and arterial and venous insufficiency were at increased risk for chronic wound infections [1]. Chronic wounds are a prime environment for bacteria, including biofilm, making wound infection a common problem [2] [3]. Managing biofilm, which can affect wound healing by creating chronic inflammation or infection [3], becomes crucial as up to 80 per cent of infections are caused by this type of bacteria [4] [5].
To adopt and integrate best practices, the team at Perley Health decided to implement the Assessment and Management of Pressure Injuries for the Interprofessional Team best practice guideline (BPG). To support a systematic approach to change, four of the action cycle phases of the Knowledge-to-Action Framework, from the Leading Change Toolkit [6] are highlighted below.
Identify the problem
Perley Health’s wound care protocol was audited and the following gaps were identified based on current evidence:
- Aseptic wound cleansing technic could be improved, as nonsterile gauze was used for wound cleansing.
- Wound cleaning solution was not effective to manage microbial load in chronic wounds
- Baseline wound infection data were collected on the number of infected wounds within the organization each month over three years and is ongoing
Adapt to local context
The project was supported by key formal and informal leaders within the organization including the Nurse Specialized in Wounds, Ostomy and continence (NSWOC), the Director of Clinical Practice, a team of wound care champions, the IPAC team and material management. Staff was motivated to improve resident outcomes by lowering infection rates which facilitated the project but many continued to use old supplies so as to not waste material. Providing the rationale for the change and associated best practices improved knowledge uptake, as did removing old supplies to cut down on confusion. Barriers the team encountered included staff turnover and educating new team members.
Select, tailor, implement interventions
The interventions listed below were selected, tailored and implemented based on the evidence that was adapted to the local context. They were purposely chosen to support the clinical teams’ needs on busy units and to creatively overcome staffing challenges. Interventions included:
- use of a wound cleanser containing an antimicrobial
- use of sterile equipment for wound care, including sterile gauze
- creation of a wound-cleansing protocol was created to reflect best practice
- updating and approval of a policy by the Risk Assessment and Prevention of Pressure Ulcers team in collaboration with the director of clinical practice
Perley Health also created and delivered education in two formats designed to be accessible to front-line staff:
- Just-in-Time education was provided on every unit, on every shift, to registered staff by the NSWOC on all shift sets, over a one-month period. Wound care champions were available on each shift to aid in learning and answer additional questions to support the team’s needs.
- A continuing education online learning module was created and uploaded onto Perley Health’s Surge learning platform. Training is included in new hire onboarding and mandatory for yearly education.
Image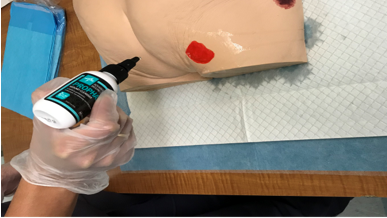
An RPN demonstrating how to cleanse a wound using wound cleanser at Perley Health
Evaluate outcomes
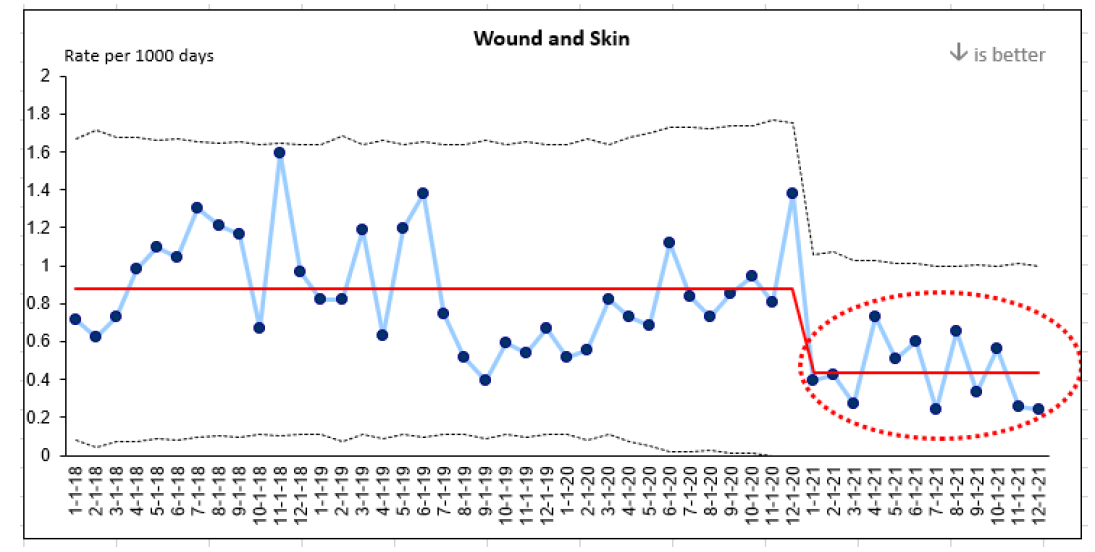
Evaluation indicators were selected to determine the impact of the implementation interventions when compared to baseline data, including the rate of wound and skin infections per 1,000 days. A 50 per cent reduction in wound infections was identified following the implementation of the identified change strategies and education above.
This graph represents four years of data collection on wound infections at Perley Health. Three years of baseline data and one year of post-implementation data are highlighted in red.
References
- Azevedo, M., Lisboa, C., & Rodrigues, A. (2020). Chronic wounds and novel therapeutic approaches. British Journal of Community Nursing, 25 (12), S26-s32.
- Landis, S.J. (2008). Chronic Wound Infection and Antimicrobial Use. Advances in Skin & Wound Care, 21 (11), p 531-540.
- Registered Nurses’ Association of Ontario (2016). Clinical best practice guidelines: Assessment and management of pressure injuries for the interprofessional team (3rd ed.). Registered Nurses’ Association of Ontario: Toronto, ON.
- Jamal, M., Ahmad, W., Andleeb, S., Jalil, F., Imran, M., Nawaz. M., Hussain, T., Ali, M., Rafiq, M., & Kamil, M.A. (2018). Bacterial biofilm and associated infections. J Chin Med Assoc. 81(1): 7-11.
- Murphy, C., Atkin, L., Swanson, T., Tachi, M., Tan, Y.K., De Ceniga, M.V., Weir, D., Wolcott, R., Ĉernohorská, J., Ciprandi, G., Dissemond, J., James, G.A., Hurlow, J., Lázaro MartÍnez, J.L., Mrozikiewicz-Rakowska, B., & Wilson, P. (2020). Defying hard-to-heal wounds with an early antibiofilm intervention strategy: wound hygiene. J Wound Care, (Sup3b):S1-S26.
- Registered Nurses’ Association of Ontario (2022). Leading change toolkit: Knowledge-to-action framework. https://rnao.ca/leading-change-toolkit Registered Nurses’ Association of Ontario: Toronto, ON.